What Is Peyronie’s Disease and Why Do So Many Men Wait Too Long to Treat It?
Peyronie’s disease is one of the most consistently underreported conditions in men’s health. Estimates suggest it affects between three and nine percent of adult men, though urologists widely believe the true prevalence is higher because so many men never bring it up with a doctor. The condition involves the formation of fibrous scar tissue, called plaque, inside the penis, which causes curvature, shortening, and in many cases pain during erection. At Lazare Urology in Brooklyn, it comes up regularly in consultations, often after a patient has been managing the condition quietly for a year or more and finally decided the impact on his life was too significant to keep ignoring.
Understanding what Peyronie’s disease actually is, how it develops, and what treatment looks like at different stages takes most of the fear out of the conversation. That conversation is worth having sooner rather than later, and this piece explains why.
What Is Actually Happening Inside the Penis
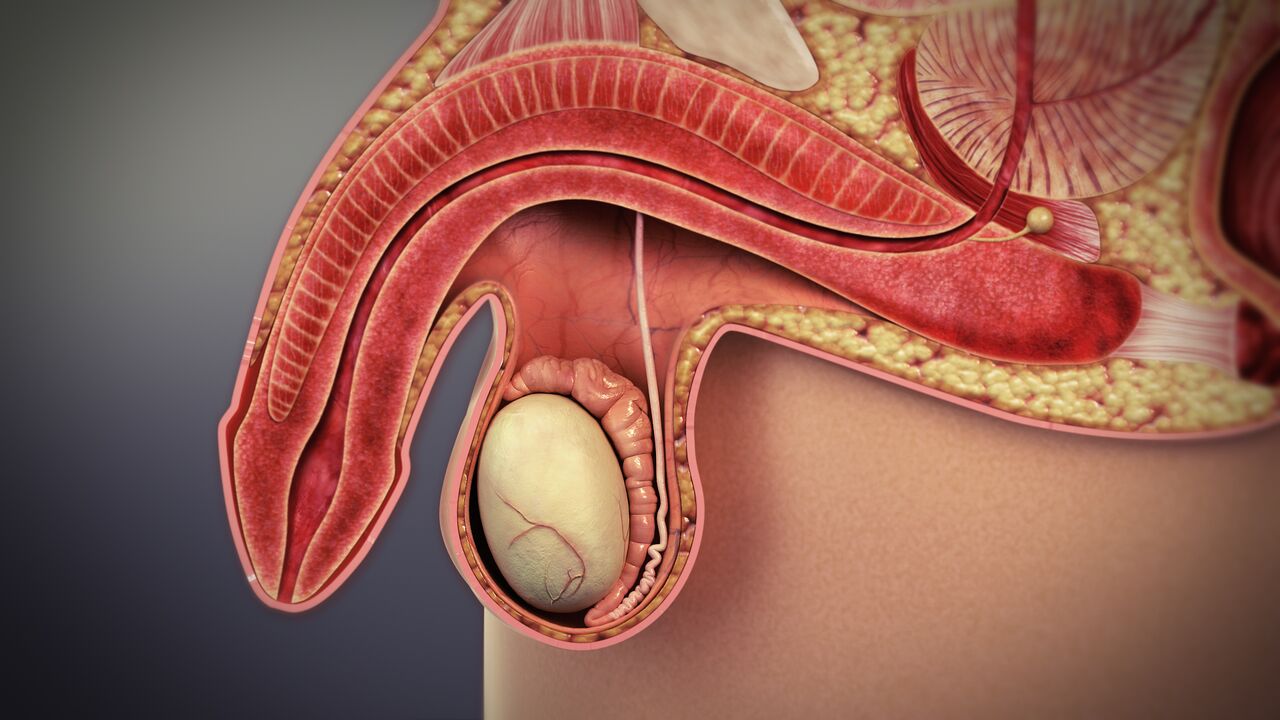
The penis contains two cylindrical chambers called the corpora cavernosa, which fill with blood during an erection and give the penis its rigidity and shape. Each chamber is encased in a tough, elastic sheath of connective tissue called the tunica albuginea. Under normal circumstances, the tunica stretches symmetrically as the penis becomes erect, allowing it to straighten and elongate.
In Peyronie’s disease, localized areas of the tunica develop fibrous plaque that does not stretch the way healthy tissue does. When the rest of the penis expands with an erection, the plaque site holds rigid, pulling the shaft toward it and creating curvature. Depending on where the plaque forms and how extensive it is, the bend can be upward, downward, to either side, or in some cases involve an hourglass or indentation deformity where the shaft narrows at the affected area rather than curving.
The condition is not, in the conventional sense, a scar from a single injury. Many men have no recollection of any trauma that could have caused it. The current understanding is that repeated microtrauma during sexual activity, combined with individual susceptibility factors including genetic predisposition, connective tissue disorders like Dupuytren’s contracture, and certain medications such as beta-blockers, can trigger an abnormal wound healing response in the tunica that produces plaque rather than normal tissue repair.
The Two Phases: Why Timing Matters for Treatment
Peyronie’s disease progresses through two distinct phases, and the distinction is clinically important because it determines which treatments are appropriate.
The acute phase is the active period, typically lasting six to eighteen months from onset. During this time, the plaque is still forming, curvature may be changing month to month, and erections are often painful. Pain during an erection is one of the clearest indicators that a man is still in the acute phase. The plaque has not yet calcified or stabilized, which means the condition is still evolving and certain treatments aimed at modifying the plaque are more likely to be useful.
The chronic phase begins when the disease has stabilized, typically defined as no change in curvature for at least three months and the resolution of pain. At this point, the plaque has matured and the deformity is what it is going to be without intervention. Surgical options become the most reliable path to meaningful correction in the chronic phase, particularly for men whose curvature is severe enough to prevent intercourse or is causing significant psychological distress.
Non-Surgical Treatment Options During the Acute Phase
The only FDA-approved non-surgical treatment for Peyronie’s disease is collagenase clostridium histolyticum, marketed under the brand name Xiaflex. This is an injectable enzyme that breaks down the collagen making up the plaque, delivered in a series of injections into the plaque itself over several treatment cycles. Clinical trials showed meaningful reductions in curvature and plaque consistency in a significant proportion of patients, with the best results seen in men with moderate curvature and palpable plaque who are still in or close to the acute phase.
Xiaflex is not appropriate for all patients. Men with severe curvature, calcified plaque, or hourglass deformities tend to see limited benefit. The injections require a trained urologist and are paired with penile modeling, a manual stretching technique performed after each injection to maximize the breaking down of the plaque. Side effects include bruising, swelling, and in rare cases corporal rupture, which is why proper patient selection and technique matter considerably.
Other non-surgical approaches, including oral vitamin E, pentoxifylline, and traction therapy using a penile extender device, have varying levels of evidence behind them. Traction therapy has shown the most consistent data for reducing curvature and preventing shortening over time and is often recommended alongside other treatments rather than as a standalone solution. Oral medications and supplements have not demonstrated reliable efficacy in well-controlled studies and are generally not a substitute for proven interventions.
Surgical Options for Chronic Peyronie’s Disease
Once the disease has stabilized, surgery offers the most predictable correction of curvature. The three main surgical approaches are plication, grafting, and penile implant placement.
Plication is the simplest option, involving sutures placed on the longer side of the penis to straighten it by shortening that side to match the plaque-affected side. It is best suited for men with mild to moderate curvature, adequate penile length, and no significant erectile dysfunction. The tradeoff is a modest reduction in penile length, which is usually small but should be understood before surgery.
Grafting procedures cut or remove the plaque and patch the resulting defect with tissue, either from the patient or from a synthetic source. This approach can correct more severe curvature without the shortening that comes with plication, but it carries a higher risk of post-operative erectile dysfunction, particularly in men who already have some degree of ED before surgery. Careful candidate selection is essential.
For men who have both Peyronie’s disease and significant erectile dysfunction that has not responded to oral medications or injection therapy, a penile implant is often the most comprehensive solution. The inflatable implant straightens the penis during placement through a manual modeling technique that breaks down the plaque, restores rigidity on demand, and addresses both conditions simultaneously. Patient satisfaction rates with this approach are consistently high, particularly among men who were dealing with the frustration of managing two interrelated problems separately.
The Psychological Weight of Waiting
The research on Peyronie’s disease consistently shows that it carries a disproportionate psychological burden relative to its physical severity. Men with the condition report high rates of depression, relationship strain, reduced self-esteem, and avoidance of sexual intimacy. Part of that burden comes from the condition itself. Part of it comes from the isolation of managing it silently and assuming it is either permanent, untreatable, or too embarrassing to discuss with a doctor.
None of those assumptions are accurate. Treatment options exist for every stage of the disease. The earlier a patient is evaluated, the more options are available. And the conversation with a urologist who treats this regularly is far less uncomfortable than most men expect it to be. Peyronie’s disease is a known, studied, treatable condition. Waiting does not make it easier to treat and often makes it worse.
Getting Evaluated at Lazare Urology in Brooklyn
A Peyronie’s disease evaluation involves a physical examination to assess the plaque location and consistency, a discussion of how the curvature has changed over time, and an assessment of erectile function. In some cases, an ultrasound is used to map the plaque and evaluate penile blood flow, which helps determine which treatment path makes the most sense.
At Lazare Urology, Dr. Jon Lazare brings surgical experience and a direct clinical approach to these consultations. Both Xiaflex injection therapy and surgical correction are available, and the recommendation reflects what the individual patient’s condition actually calls for rather than a one-size-fits-all approach. For men in Brooklyn and across the New York area who have been putting this off, the consultation is the straightforward first step that most patients wish they had taken earlier.
Contact Lazare Urology today to schedule an evaluation and get a clear picture of where your condition stands and what your options are.




-
What Is Peyronie’s Disease and Why Do So Many Men Wait Too Long to Treat ...
Peyronie’s disease is one of the most consistently underreported conditions in men’s ... -
-
-


